
H1N1 Vaccine Highest Risk Last?
Highest mortality groups last in line for H1N1 vaccine sets the stage for this enthralling narrative, offering readers a glimpse into a crucial chapter of pandemic history. This article delves into the historical distribution strategies, examining the rationale behind prioritizing certain groups and the challenges faced during the H1N1 pandemic. We’ll analyze the factors that influenced vaccination order, scrutinize the demographics and health conditions associated with higher mortality rates, and explore the ethical implications of prioritizing some groups over others.
The impact on public health and alternative strategies for equitable vaccine distribution will also be discussed.
Understanding the complexities of vaccine allocation during a pandemic is critical. This in-depth look at the H1N1 vaccine rollout offers valuable insights into the challenges and considerations involved in such a crucial public health undertaking. From the historical context to the potential consequences of delayed vaccination, the narrative explores the ethical dilemmas and public health implications.
Background on H1N1 Vaccine Distribution
The 2009 H1N1 pandemic, also known as swine flu, highlighted the critical need for efficient and equitable vaccine distribution strategies. Understanding the historical context and challenges surrounding the initial rollout of the vaccine is essential to improving future pandemic responses. This involves analyzing the rationale behind prioritization, the difficulties encountered during distribution, and the diverse approaches adopted by different nations.The rapid spread of the H1N1 virus necessitated a swift and coordinated response.
Vaccine production and distribution were crucial aspects of this response, as the virus posed a serious threat to public health. Effective strategies were needed to ensure equitable access to the vaccine and to prevent the spread of misinformation and distrust.
Historical Overview of H1N1 Vaccine Distribution Strategies
The H1N1 pandemic of 2009 presented unprecedented challenges in vaccine distribution. Prioritization strategies were crucial to ensure the most vulnerable populations received the vaccine first. These strategies were developed to mitigate the spread of the virus and safeguard high-risk groups.
Rationale Behind Prioritizing Certain Groups for Vaccination
High-risk groups, including pregnant women, young children, the elderly, and individuals with underlying health conditions, were prioritized for vaccination. This prioritization was based on the increased susceptibility and severity of illness in these groups. The rationale stemmed from the understanding that these populations would experience a disproportionately high risk of severe outcomes if infected.
Challenges Faced in Vaccine Distribution During the H1N1 Pandemic
Several challenges hindered the effective distribution of the H1N1 vaccine. These challenges included limited vaccine supply, varying logistical capabilities across different countries, and the emergence of public health concerns regarding the vaccine’s safety and efficacy. Ensuring sufficient vaccine supplies was crucial for a timely and comprehensive vaccination program.
Factors Influencing the Order of Vaccination
Several factors influenced the order of vaccination, including the severity of the disease in various groups and the available vaccine supply. The availability of resources, such as healthcare infrastructure and trained personnel, played a critical role in the vaccine rollout. Public health recommendations, safety concerns, and the pace of vaccine production also had an impact.
Timeline of Vaccine Rollout and Distribution
| Date | Event |
|---|---|
| April 2009 | H1N1 pandemic declared |
| May 2009 | Initial vaccine production begins |
| June-August 2009 | Vaccine distribution to high-risk groups commences |
| September 2009 | Wider vaccination campaigns launched |
| October 2009 | Increased vaccine production to meet demand |
Comparison of Different Countries’ Approaches to H1N1 Vaccine Distribution
Different countries employed various approaches to vaccine distribution. These approaches varied based on factors like national healthcare infrastructure, public health resources, and the severity of the pandemic within each country.
| Country | Prioritization Strategy | Distribution Channels | Challenges |
|---|---|---|---|
| United States | Prioritization based on risk factors and healthcare worker status | Through healthcare facilities and mass vaccination clinics | Vaccine supply shortages and public skepticism |
| Canada | Prioritization focused on high-risk individuals and essential workers | Through pharmacies and healthcare providers | Limited vaccine supply and logistical challenges |
| United Kingdom | Prioritization based on age and health conditions | Through general practices and vaccination centers | Vaccine hesitancy and concerns about efficacy |
Understanding Mortality Groups
The H1N1 pandemic highlighted the disproportionate impact of influenza on vulnerable populations. Understanding the specific demographics and health conditions associated with higher mortality rates is crucial for targeted prevention and treatment strategies. This knowledge allows for better allocation of resources and interventions to those most at risk.
Demographics Associated with Higher Mortality
Certain demographic groups exhibited heightened susceptibility to severe H1N1 outcomes. Age, particularly in the very young and the elderly, played a significant role. Pre-existing medical conditions also significantly increased the risk of severe illness and death. This understanding allows for tailored public health messaging and vaccine prioritization.
Health Conditions Increasing H1N1 Vulnerability
Several pre-existing health conditions significantly increased the risk of severe H1N1 infection. These conditions often compromised the immune system’s ability to fight off the virus, leading to complications and a higher mortality rate. Chronic respiratory illnesses, such as asthma and cystic fibrosis, were frequently associated with severe outcomes. Diabetes, a condition characterized by high blood sugar, was also linked to increased susceptibility to severe H1N1 complications.
Individuals with weakened immune systems, including those undergoing chemotherapy or organ transplant recipients, were at substantial risk.
Severity of H1N1 Illness Across Age Groups
The severity of H1N1 illness varied significantly across different age groups. Infants and young children, along with the elderly, often experienced more severe complications, including pneumonia and respiratory distress syndrome. This is due to their immature or weakened immune systems. Adults in their prime generally experienced less severe symptoms. However, those with pre-existing conditions, regardless of age, were at higher risk for serious outcomes.
Table: Mortality Groups and Associated Risk Factors
| Mortality Group | Associated Risk Factors |
|---|---|
| Infants and Young Children | Immature immune systems, underdeveloped respiratory systems, and potential for rapid deterioration. |
| Elderly (65+) | Weakened immune systems, chronic diseases (e.g., heart disease, diabetes, respiratory conditions), and age-related decline in organ function. |
| Individuals with Chronic Respiratory Conditions | Asthma, cystic fibrosis, chronic bronchitis, and other conditions that compromise lung function. |
| Individuals with Chronic Cardiovascular Conditions | Heart disease, high blood pressure, and other conditions that weaken the cardiovascular system. |
| Individuals with Diabetes | Impaired immune response and increased susceptibility to infections. |
| Individuals with Weakened Immune Systems | Organ transplant recipients, patients undergoing chemotherapy, and individuals with HIV/AIDS. |
Scientific Evidence Supporting High-Risk Groups
Numerous epidemiological studies and clinical trials during and after the H1N1 pandemic confirmed the increased risk of severe illness and death in the groups mentioned. These studies often observed higher rates of hospitalization and mortality in individuals with the conditions listed above. Extensive data analysis revealed clear correlations between specific conditions and heightened vulnerability to H1N1. For instance, studies consistently demonstrated a significant association between diabetes and increased risk of severe H1N1 complications.
Examining the “Last in Line” Phenomenon: Highest Mortality Groups Last In Line For H1n1 Vaccine
The H1N1 pandemic highlighted stark inequalities in access to crucial resources, particularly healthcare interventions like vaccines. This uneven distribution, often placing certain mortality groups at the tail end of vaccine rollout, raises critical questions about equity and fairness in public health emergencies. Understanding these disparities is essential for improving future responses to pandemics and ensuring equitable access to life-saving resources.The concept of “last in line” refers to the phenomenon where specific mortality groups, often characterized by pre-existing health conditions or socioeconomic factors, were not prioritized for vaccination during the H1N1 pandemic.
It’s frustrating to see vulnerable populations, like those with the highest mortality risk, often placed last in line for crucial vaccines like H1N1. Meanwhile, tech giants like Microsoft are constantly battling server issues, and recently, they successfully squashed some serious bugs, showcasing their commitment to reliable systems. This is a great example of how important it is to ensure everyone, especially those in high-risk groups, has equal access to vital healthcare resources.
microsoft stomps beastly server bugs highlights the need for similar focus on equitable access to essential resources, including vaccines for the most vulnerable.
This delayed access could have significant and lasting consequences on public health outcomes.
Examples of Delayed Vaccination
The delayed vaccination of pregnant women, individuals with chronic respiratory illnesses, and the elderly exemplifies the “last in line” phenomenon. Limited resources and logistical challenges in vaccine distribution played a significant role in these delays. Further, the lack of clear prioritization guidelines and insufficient communication strategies contributed to the uneven distribution of vaccines. These delays were not isolated incidents; they were observed across various regions and healthcare systems.
Potential Reasons for Delayed Access
Several factors likely contributed to the delayed access to vaccines for vulnerable populations. Limited vaccine supply was a significant constraint. The rapid spread of the virus, combined with the need to prioritize groups at high risk of severe illness, led to initial prioritization based on factors like age and existing medical conditions. However, a lack of clarity on the relative risk levels across different mortality groups and inadequate communication strategies resulted in delayed vaccination for some vulnerable populations.
Ethical Implications of Prioritization
Prioritizing certain groups over others during a pandemic raises significant ethical considerations. The principle of justice and equity demands that everyone has equal access to life-saving interventions. The prioritization decisions during the H1N1 pandemic sparked ethical debates about fairness, accountability, and the responsibility of healthcare systems to protect all vulnerable populations. A thorough ethical framework for resource allocation in public health emergencies is crucial to prevent similar injustices in the future.
Public Health Consequences of Delayed Vaccination
Delayed vaccination for mortality groups can have substantial negative public health consequences. Increased morbidity and mortality rates in these groups could have been avoided with timely vaccination. Furthermore, the delayed vaccination strategy might have had an indirect impact on the overall control of the pandemic. The delayed vaccination of high-risk groups potentially hindered herd immunity, increasing the overall risk of transmission.
Socioeconomic Factors Contributing to the Phenomenon
Socioeconomic factors, such as access to healthcare, transportation, and communication, played a significant role in determining the extent to which specific mortality groups were affected by delayed access to vaccines. Individuals with limited access to resources might have been disproportionately affected by logistical challenges and communication gaps in the vaccine rollout. The pandemic highlighted the existing health disparities that exacerbate the impact of public health emergencies on vulnerable populations.
Comparison of Vaccination Access Across Mortality Groups
| Mortality Group | Vaccination Prioritization | Potential Challenges |
|---|---|---|
| Pregnant women | Often lower priority initially | Concerns about potential risks of vaccination during pregnancy |
| Individuals with chronic respiratory illnesses | Potentially delayed due to perceived higher risk | Coordination and accessibility to vaccination sites for those with mobility limitations |
| Elderly | Often prioritized but may have experienced delays | Limited mobility, communication barriers, and potentially lower trust in healthcare systems |
| Low-income communities | Potentially disadvantaged due to lack of access to information and healthcare resources | Transportation difficulties, lack of awareness, and mistrust of healthcare systems |
Impact on Public Health
The H1N1 pandemic highlighted the crucial importance of equitable vaccine distribution, especially for vulnerable populations. Prioritizing individuals at higher risk of severe illness or death is a cornerstone of effective pandemic response. However, delays in vaccine access for mortality groups can have far-reaching and detrimental consequences, affecting not only the immediate health of those individuals but also the broader public health landscape.The delayed vaccination of mortality groups during the H1N1 pandemic resulted in a disproportionate burden of illness and death within these populations.
This unequal access to preventive measures exacerbated existing health disparities and demonstrated the critical need for more robust and equitable vaccine allocation strategies.
Potential Consequences of Delayed Vaccination for Mortality Groups
Delayed vaccination for mortality groups, such as those with underlying health conditions, can lead to a higher incidence of severe H1N1 complications and death. This is particularly true for individuals with chronic respiratory illnesses, compromised immune systems, and other conditions that make them more susceptible to the virus’s effects. The lack of prompt access to preventive measures can result in increased hospitalization rates, prolonged recovery periods, and higher mortality rates compared to those who received the vaccine promptly.
The heartbreaking reality of the H1N1 vaccine rollout, with highest mortality groups often last in line, raises serious questions about equitable access to vital resources. This echoes the current digital content landscape, where aggressive moves like Hulu’s expansion seem to be the first salvo in a larger war for viewers. This strategic approach, detailed in the article “is Hulu’s heave-ho first salvo in digital content war” is Hulu’s heave ho first salvo in digital content war , highlights the complexities of prioritizing resources, a critical issue also present in the H1N1 vaccine rollout.
Impact on Overall H1N1 Transmission and Mortality Rates
The delayed vaccination of mortality groups can contribute to a prolonged period of H1N1 transmission. A substantial segment of the population remains unvaccinated, and this unvaccinated population can serve as reservoirs for the virus. This prolonged circulation can result in the emergence of new strains or variants, potentially leading to more severe outcomes. Delayed vaccination can also lead to a slower decline in overall H1N1 mortality rates, impacting public health efforts to control the pandemic.
Long-Term Health Effects on Individuals Not Prioritized for Vaccination
Individuals not prioritized for vaccination, especially those in mortality groups, might experience long-term health complications from the H1N1 infection. This can manifest as chronic respiratory problems, neurological disorders, and other long-lasting conditions. The severity of these conditions varies, and some individuals may experience lingering effects for extended periods, significantly impacting their quality of life.
Lessons Learned from the H1N1 Pandemic Regarding Vaccine Allocation
The H1N1 pandemic underscored the importance of comprehensive risk assessment and prioritization in vaccine allocation. The experience revealed that a more equitable and transparent distribution system is essential to protect the most vulnerable populations. The need for real-time data on virus transmission, severity of cases, and vaccine supply is crucial to adjusting strategies effectively.
How This Situation Affected Vaccine Confidence and Trust
The uneven distribution of H1N1 vaccines can negatively affect public trust and confidence in the vaccination process. The perception of inequity in access can lead to vaccine hesitancy, making it more challenging to achieve herd immunity and control the spread of the virus. This lack of trust can also create a barrier to public health interventions in future outbreaks.
Overall Impact of Vaccination Strategies on Different Mortality Groups
| Mortality Group | Vaccination Strategy Impact |
|---|---|
| Individuals with chronic respiratory illnesses | Delayed vaccination significantly increases the risk of severe complications and death. |
| Individuals with compromised immune systems | Delayed vaccination results in increased susceptibility to severe H1N1 infections. |
| Pregnant women | Delayed vaccination may have adverse effects on both the mother and the fetus. |
| Children | Delayed vaccination can lead to increased transmission and potentially severe outcomes in this vulnerable group. |
Alternative Vaccination Strategies
The H1N1 pandemic highlighted the critical need for more equitable and efficient vaccine distribution strategies. Simply prioritizing certain groups based on mortality risk, while understandable, can create inequities and potentially miss opportunities to protect vulnerable populations. Alternative models for vaccine allocation are crucial to minimize the impact of future pandemics and ensure broader community protection.
Alternative Models for Vaccine Allocation
Several alternative models for vaccine allocation can be considered, each with its own strengths and weaknesses. These models move beyond a strict risk-based approach, aiming for broader protection and potentially reducing the societal impact of future outbreaks.
Hypothetical Scenario for Equitable Distribution
Imagine a hypothetical scenario where a new influenza strain emerges. Instead of prioritizing high-mortality groups first, the allocation strategy incorporates factors like occupation (healthcare workers, essential personnel), household composition (individuals with young children or elderly relatives), and geographic location (areas with high population density or limited access to healthcare). This approach recognizes that factors beyond mortality risk contribute to the spread and severity of outbreaks.
Furthermore, this model considers the interconnectedness of different communities and the importance of maintaining societal function.
Examples of Other Pandemics, Highest mortality groups last in line for h1n1 vaccine
The SARS outbreak of 2003 demonstrated the complexities of vaccine allocation when faced with a novel pathogen. Similarly, the 2014-2016 Ebola outbreak highlighted the importance of community engagement and tailored strategies to address specific cultural and social factors within affected regions. These events underscore the need for adaptable and context-sensitive vaccine allocation models.
Comparison of Vaccination Strategies
Various vaccine allocation strategies have different levels of effectiveness. A purely risk-based approach may miss crucial opportunities to protect those at high risk of transmission, whereas a broader, more equitable approach might be more effective in preventing widespread outbreaks. Ultimately, the optimal strategy depends on the specific characteristics of the pandemic, including the severity of the disease, transmission rate, and the capacity of the healthcare system.
It’s frustrating that high-risk groups for H1N1 often get the vaccine later, as if their lives matter less. This unequal access to critical resources seems absurd, especially when considering how presidents have historically interacted with technology, like how President Obama surprisingly held onto Blackberry phones for a long time, as seen in this interesting article. Ultimately, prioritizing vulnerable populations for vaccinations should be a top priority, not an afterthought.
The delayed rollout of the vaccine to these groups is a serious public health concern.
Advantages and Disadvantages of Prioritization Models
Different prioritization models offer distinct advantages and disadvantages. For example, a model prioritizing healthcare workers might be beneficial in preventing the collapse of the healthcare system, but might not adequately address the needs of other vulnerable groups. Conversely, a model that considers household composition might better protect children and the elderly, but could be more complex to implement.
The trade-offs between various strategies must be carefully considered.
Vaccination Strategies: A Comparative Table
| Vaccination Strategy | Pros | Cons |
|---|---|---|
| Risk-Based (Mortality Focus) | Simple to implement, prioritizes those at highest risk of severe outcomes. | May not adequately address the needs of vulnerable populations, can lead to disparities. |
| Equitable Allocation (Broader Criteria) | Aims to protect a larger portion of the population, potentially reducing community transmission. | More complex to implement, may require more resources and data. |
| Prioritization by Occupation | Protects essential services, potentially limiting the disruption to critical infrastructure. | May overlook other vulnerable populations, could lead to inequities. |
| Geographic Targeting | Addresses the needs of specific communities with high risk or limited resources. | May not account for transmission patterns, may exacerbate existing inequalities. |
Illustrative Examples of H1N1 Mortality Data
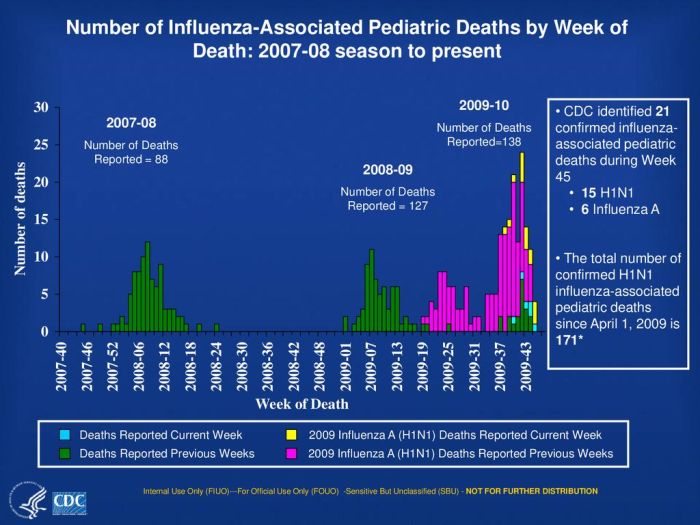
The H1N1 pandemic of 2009 highlighted the significant disparities in mortality rates across different demographic groups. Understanding these patterns is crucial for developing targeted public health interventions and resource allocation. This analysis delves into illustrative examples of mortality data, focusing on specific demographic factors and health conditions associated with increased risk.This exploration reveals the complexity of the H1N1 pandemic, emphasizing the need for a nuanced understanding of risk factors beyond simple demographics.
The aim is to illustrate the data, not to provide a complete epidemiological analysis.
Mortality Rates by Age Group
Age was a strong predictor of H1N1 mortality. Individuals at the extremes of the age spectrum, both very young children and the elderly, experienced disproportionately higher mortality rates compared to those in the middle age groups. This vulnerability is likely due to factors such as underdeveloped or weakened immune systems in young children and the presence of underlying health conditions common among the elderly.
This observation underscores the importance of vaccination strategies that target these vulnerable populations.
- Children under 5 years old and adults aged 65 and older had significantly higher mortality rates compared to those in the middle age ranges. This is likely due to a combination of factors, including differences in immune responses and the prevalence of underlying health conditions.
Mortality Rates by Pre-existing Health Conditions
Individuals with pre-existing health conditions, such as asthma, diabetes, and chronic respiratory illnesses, were at an elevated risk of severe H1N1 infection and death. These conditions often compromised the immune system’s ability to fight off the virus, leading to more serious complications. The data highlighted the critical role of underlying health conditions in determining the severity of H1N1 infections.
- Individuals with chronic respiratory illnesses, such as asthma and chronic obstructive pulmonary disease (COPD), had higher mortality rates than those without these conditions. This suggests a significant impact of respiratory system vulnerability on the outcome of H1N1 infections.
- Diabetics were also a higher-risk group. High blood sugar levels can impair the immune response, making individuals more susceptible to severe illness and death from the virus.
Mortality Rates by Ethnicity
While significant disparities in mortality rates existed, the specific patterns related to ethnicity were complex and multifaceted. Data often revealed higher mortality rates in certain ethnic groups, but the underlying causes were rarely straightforward. Factors such as socioeconomic status, access to healthcare, and pre-existing health conditions often played significant roles. The analysis necessitates further investigation into the complex interplay of factors contributing to these disparities.
- In some studies, certain ethnic groups displayed higher mortality rates compared to others. This observation highlights the need for a comprehensive understanding of the contributing factors, including socioeconomic factors, access to healthcare, and potential underlying health conditions.
Infographic Representation
A hypothetical infographic could visually represent the distribution of H1N1 cases and mortality rates across different demographics. The infographic might use stacked bar charts to compare mortality rates between age groups, pre-existing conditions, and ethnic groups. A color-coded system could be used to highlight different demographic categories, and the y-axis could display the mortality rates. The infographic would effectively communicate the key findings from the data.
Final Review
In conclusion, the H1N1 vaccine rollout highlights the critical need for equitable and effective vaccine allocation strategies during public health crises. The experiences from this pandemic offer invaluable lessons for future pandemics and underscore the importance of considering the unique needs and vulnerabilities of high-mortality groups. This article has explored the factors that contributed to the “last in line” phenomenon, emphasizing the ethical implications and potential consequences for public health.
Alternative strategies for vaccine allocation are also presented, encouraging a more comprehensive approach to future public health crises.